- Jun 3
Combination Therapy for Leg Spider Veins
- Haroun Gajraj
Why RF Thermocoagulation and Microsclerotherapy Work Better Together
Dr Haroun Gajraj | VeinCare Academy | www.veincare.academy
There is one treatment that works brilliantly for spider veins on the face. And there is one treatment that works brilliantly for spider veins on the legs. They are not the same treatment.
But here is what the published literature now confirms: combining both treatments — on the legs, in a single patient pathway — produces better results than either modality can achieve alone. The patients who benefit most are those with exactly the kind of veins that practitioners have always found the hardest to treat.
This article explains the evidence, the biological rationale, and what a practical clinical protocol looks like.
🎥 Prefer video? Watch the full 16-minute clinical guide on YouTube: "The New Gold Standard for Leg Spider Veins? Sclerotherapy vs. RF Thermocoagulation" →
Two Gold Standards
RF Thermocoagulation for Facial Telangiectasias
On the face, radiofrequency (RF) thermocoagulation at 4 MHz is the established treatment of choice for fine telangiectasias — the tiny red thread veins across the nose and cheeks. A fine insulated probe pierces the epidermis and rests on the vessel wall. A brief half-second to one-second pulse of 4 MHz current heats the vessel to coagulation temperature, the wall denatures, and the vessel obliterates and is absorbed.
The rationale for preferring RF over sclerotherapy on the face is compelling. Facial telangiectasias are typically too fine to inject reliably. More importantly, sclerotherapy on the face carries serious risks that do not apply on the legs: cutaneous necrosis from inadvertent intra-arterial injection, persistent post-inflammatory hyperpigmentation, and — in rare but reported cases — visual complications including blindness from retrograde arterial embolisation of sclerosant. RF thermocoagulation bypasses all of these risks. There is no sclerosant, no injection, and no medication entering the systemic circulation.
The published clinical experience with this approach is substantial. Jean-Marc Chardonneau (2018), in the International Journal of Clinical & Experimental Dermatology, reported outcomes across thousands of RF treatments for telangiectasias. For leg telangiectasias, Chardonneau reported approximately 75% positive outcomes, and 85% for ankle and foot vessels, with a single treatment session.
Microsclerotherapy for Leg Spider Veins
On the legs, the anatomy and haemodynamics are different. Leg telangiectasias and reticular veins are larger, more numerous, fed by dermal feeder vessels under moderate hydrostatic pressure. Microsclerotherapy — injecting a small volume of sclerosant directly into the target vessel — has been the gold standard for decades.
The evidence base is robust. The 2021 Cochrane systematic review by Nakano et al. (Cochrane Database Syst Rev. 2021;10:CD012723) examined 35 randomised controlled trials involving 3,632 participants. It confirmed that sclerotherapy agents are significantly more effective than placebo for resolution of telangiectasias (SMD 3.08, 95% CI 2.68–3.48; moderate-certainty evidence), and that sclerotherapy remains the most effective single modality for leg C1 vein disease overall. Notably, the review found no studies investigating thermocoagulation, identifying this as a significant gap in the literature.
Sclerotherapy works particularly well for reticular veins — the blueish feeder vessels typically 1–3 mm in diameter — and for spider veins large enough to cannulate reliably. So the question stands: if sclerotherapy is the gold standard, why would you add anything else?
The Problem Sclerotherapy Cannot Fully Solve
The answer lies in a subset of leg telangiectasias that falls outside the optimal treatment envelope for sclerotherapy — the very finest vessels, typically less than 0.5 mm in diameter.
The Technical Challenge of Fine Vessel Injection
Getting a needle tip into a vessel under half a millimetre across, in the superficial dermis, is technically demanding even for experienced practitioners. An extravascular injection of sclerosant produces a dermal wheal, triggers local inflammation, risks blistering and scab formation, and — in the worst case — can produce cutaneous necrosis. The finer the vessel and the more superficial it sits, the narrower the margin for error.
Hyperpigmentation and Haemosiderin Staining
Even when sclerotherapy is performed accurately in fine telangiectasias, the inflammatory response to endothelial destruction releases haemoglobin into the perivascular dermis. This degrades to haemosiderin — an iron-containing pigment producing the characteristic brown staining known as post-sclerotherapy hyperpigmentation (PSH).
The incidence and histological basis of PSH are well-established. Goldman, Kaplan and Duffy (1987) (J Dermatol Surg Oncol. 1987;13(5):547–550) established that PSH represents haemosiderin deposition — not melanocytic change — and occurs in 10–30% of patients following sclerotherapy of vessels between 0.1 and 5 mm. Eighty percent of patients clear spontaneously within 6–24 months; a minority experience persistence for up to five years. A more recent histopathological study, Bossart et al. (2025) (Phlebology, DOI: 10.1177/02683555251357095), confirmed that both haemosiderin and post-inflammatory dermal melanin contribute to PSH, with haemosiderin predominating in newer lesions.
Telangiectatic Matting
Telangiectatic matting — the post-treatment appearance of new fine vessels (under 0.2 mm diameter) around the treated area — is a recognised and frustrating complication of sclerotherapy. Goldman, Sadick and Weiss (1995) (Dermatol Surg. 1995;21(1):19–29) established the incidence at approximately 15–20% of patients treated by sclerotherapy, attributing the mechanism to reactive inflammatory and angiogenic responses. The retrospective analysis by Davis and Duffy (1990) (J Dermatol Surg Oncol. 1990;16(4):327–330), reviewing 2,120 patients, found an overall incidence of 16%, with significantly higher rates in patients who were overweight, on hormonal therapy, or had a family history of telangiectasia (p < 0.05).
Recurrence from Inadequately Treated Feeders
Venous pressure from untreated reticular feeders rapidly repopulates treated fine vessels. Without adequate destruction of the feeding reticular network, recurrence is predictable.
The net result is a clinically significant cohort — patients with fine telangiectasias that cannot be safely injected, those who develop matting or pigmentation after injection of fine vessels, and those with recurrent fine vessels after multiple treatment courses. These are the patients who return after their second or third session asking why those particular veins persist.
Why Combination Therapy Makes Biological Sense
The combination approach addresses this problem by deploying each modality within its optimal vessel size range — a division of labour based on vessel calibre.
Reticular veins (1–3 mm, mid-dermis, moderate pressure): ideal targets for sclerotherapy. 0.5% polidocanol liquid contacts the endothelium, initiates fibrotic obliteration, and the vessel is absorbed over subsequent weeks.
Fine spider veins (under 0.5 mm, superficial dermis, low pressure): ideal targets for RF thermocoagulation at 4 MHz. The probe coagulates the vessel wall without injection, without sclerosant, and without the haemosiderin deposition that drives PSH.
The histological basis for this division is directly evidenced. Bush and Bush (2018) (J Cosmet Dermatol. 2018;17(5):779–782) treated 135 patients with ohmic thermolysis (RF thermocoagulation), 940 nm laser, or 940 nm laser combined with sclerotherapy. Skin biopsies at 4–6 weeks post-treatment showed that ohmic thermolysis produces electrodesiccation of the squamous epithelium, reticular dermis, and fusion of the target vessel, with vessel clearance of over 90% in telangiectasias under 0.5 mm — the precise size range where sclerotherapy carries disproportionate risk. No long-term skin sequelae were observed at recommended device settings.
The Randomised Controlled Trial Evidence
The question — does adding RF thermocoagulation to sclerotherapy improve outcomes compared with sclerotherapy alone? — has been directly tested in a randomised trial. Diken et al. (2021) published a pilot RCT in Phlebology (2021;36(8):620–626; DOI: 10.1177/02683555211006534). 111 patients with leg telangiectasias (CEAP C1) were randomised to sclerotherapy alone (Group 1) or sclerotherapy immediately followed by low-energy percutaneous RF thermocoagulation (Group 2). Results across all outcome measures favoured the combination:
Cosmetic improvement scores (self-assessed) were significantly higher in the combination group (p = 0.001)
Hyperpigmentation was significantly lower in the combination group (p = 0.009)
Trapped blood was significantly lower in the combination group (p = 0.02)
Fewer treatment sessions were required to achieve the cosmetic endpoint
-
No additional complications were observed — the combination added benefit without adding risk
As a pilot RCT, this trial was designed to establish feasibility and generate preliminary data for a larger definitive study. The sample size and statistical power are accordingly limited. Results should be regarded as hypothesis-generating rather than practice-defining in isolation. Nevertheless, this remains the only randomised trial to have directly addressed this specific comparison, and it points consistently in one direction: the combination outperforms monotherapy with no additional risk profile.
Head-to-Head: RF vs Sclerotherapy for Fine Veins
Complementary comparative data are provided by Korolova et al. (2023) (Wiad Lek. 2023;76(9):1992–1999; DOI: 10.36740/WLek202309113), who randomised 52 patients to RF thermocoagulation or sclerotherapy. Both treatments significantly improved quality of life (p < 0.001 for both groups). However, RF thermocoagulation showed a significantly greater impact on quality of life (p = 0.003). Average spider vein length in the treatment area decreased by 92.1% with RF compared with 73.4% with sclerotherapy (p < 0.01). The authors' conclusion: radiofrequency coagulation better eliminates small veins less than 0.3 mm — the precise vessel calibre range targeted in the combination approach.
The Evidence Gap
The 2021 Cochrane review by Nakano et al. — 35 RCTs, 3,632 participants — is the most comprehensive systematic review of treatment for telangiectasias and reticular veins. It did not include RF thermocoagulation as a comparator in its primary analysis, explicitly noting that no studies investigated thermocoagulation. This is not a negative finding; it is an evidence gap. The combination approach remains without a large, adequately powered, multi-centre RCT.
This gap is unlikely to be closed soon. Large RCTs in procedural phlebology are resource-intensive, difficult to blind, and rarely commercially funded. Clinicians adopting the combination approach should do so on the basis of its biological rationale, the preliminary RCT data from Diken et al., the comparative data from Korolova et al., and their own clinical judgment — not on the assumption that definitive large-scale evidence exists.
A Practical Clinical Protocol
Option 1: Sequential Treatment (Recommended for Extensive Reticular Disease)
Session 1: Microsclerotherapy targeting reticular feeder veins with 0.5% polidocanol liquid. Treat any directly injectable spider veins at the same session with 0.25% polidocanol.
Wait 4–6 weeks for the post-sclerotherapy inflammatory response to resolve and vessel obliteration to proceed.
-
Session 2: RF thermocoagulation at 4 MHz for residual fine spider veins (< 0.5 mm) that either did not respond to sclerotherapy or were too fine to inject initially. This phase typically takes 10–20 minutes.
Option 2: Single-Session Combination
Sclerotherapy and RF thermocoagulation performed in the same visit. Reticular veins and injectable spider veins are treated with sclerotherapy; fine vessels are treated simultaneously with RF. The advantage is fewer patient visits. The session is longer, but compression applies only to the sclerotherapy-treated vessels.
The choice between options depends on the extent of reticular disease, the proportion of very fine vessels, and patient preference regarding visit frequency. In patients with predominantly fine spider veins and minimal reticular disease, a single-session RF-dominant approach may be most efficient.
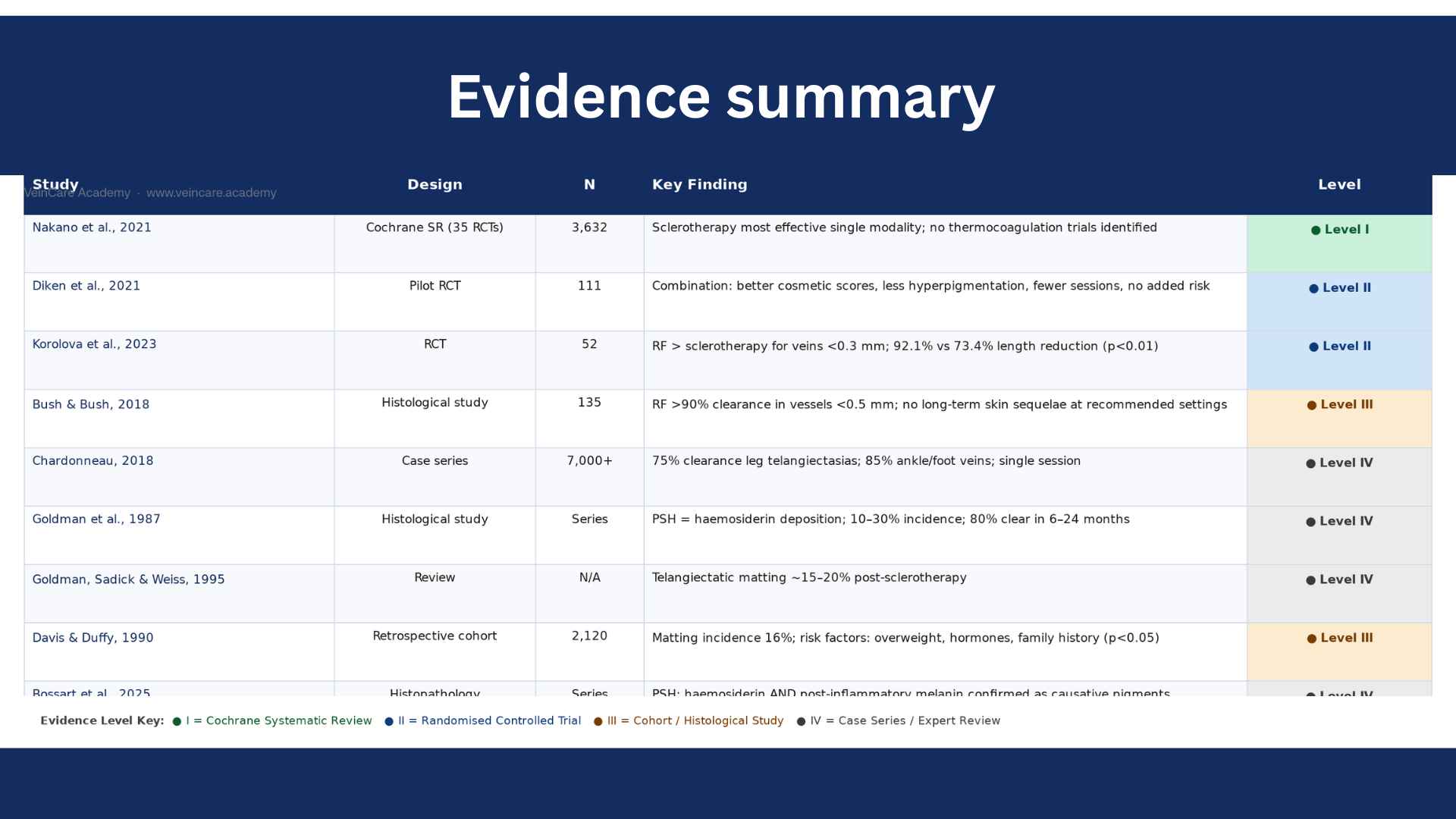
Evidence Summary
Clinical Takeaways
Sclerotherapy remains the most evidence-based single treatment for leg telangiectasias (Level I Cochrane evidence; Nakano et al., 2021).
RF thermocoagulation at 4 MHz achieves over 90% vessel clearance in telangiectasias under 0.5 mm — where sclerotherapy carries the highest risk of hyperpigmentation and telangiectatic matting (Bush & Bush, 2018).
The only RCT directly testing the combination (Diken et al., 2021; N=111) found significantly better cosmetic outcomes, less hyperpigmentation, and fewer treatment sessions versus sclerotherapy alone, with no additional complications.
RF is superior to sclerotherapy specifically for vessels under 0.3 mm (Korolova et al., 2023; 92.1% vs 73.4% reduction, p<0.01).
The combination is biologically rational: sclerotherapy for reticular feeders (1–3 mm); RF for fine spider veins (< 0.5 mm).
-
A large definitive RCT for this combination has not yet been published. Adoption is ahead of the formal evidence base but consistent with its biological rationale and current preliminary trial data.
References
1. Nakano LCU, Cacione DG, Baptista-Silva JCC, Flumignan RLG. Treatment for telangiectasias and reticular veins. Cochrane Database Syst Rev. 2021;10(10):CD012723. doi: 10.1002/14651858.CD012723.pub2. [PubMed/Source →]
2. Diken AI, Alemdaroğlu U, Özyalçın S, et al. Adjuvant radiofrequency thermocoagulation improves the outcome of liquid sclerotherapy in the treatment of spider veins of the leg: a pilot study. Phlebology. 2021;36(8):620–626. doi: 10.1177/02683555211006534. [PubMed/Source →]
3. Korolova K, Korolova Z, Teplyi V, Sydorenko R. Mini-invasive treatment methods of spider veins: sclerotherapy and radiofrequency thermocoagulation. Wiad Lek. 2023;76(9):1992–1999. doi: 10.36740/WLek202309113. [PubMed/Source →]
4. Bush RG, Bush P. Histological findings correlated with clinical outcomes in telangiectasia treated with ohmic thermolysis and 940 nm laser. J Cosmet Dermatol. 2018;17(5):779–782. doi: 10.1111/jocd.12761. [PubMed/Source →]
5. Chardonneau JM. Radiofrequency and Telangiectasias. Int J Clin Exp Dermatol. 2018;3(2):3–5. [PubMed/Source →]
6. Goldman MP, Kaplan RP, Duffy DM. Postsclerotherapy hyperpigmentation: a histologic evaluation. J Dermatol Surg Oncol. 1987;13(5):547–550. doi: 10.1111/j.1524-4725.1987.tb00940.x. [PubMed/Source →]
7. Goldman MP, Sadick NS, Weiss RA. Cutaneous necrosis, telangiectatic matting, and hyperpigmentation following sclerotherapy: etiology, prevention, and treatment. Dermatol Surg. 1995;21(1):19–29. doi: 10.1111/j.1524-4725.1995.tb00107.x. [PubMed/Source →]
8. Davis LT, Duffy DM. Determination of incidence and risk factors for postsclerotherapy telangiectatic matting of the lower extremity: a retrospective analysis. J Dermatol Surg Oncol. 1990;16(4):327–330. doi: 10.1111/j.1524-4725.1990.tb00043.x. [PubMed/Source →]
9. Bossart S, Ramelet AA, Seyed Jafari SM, et al. Revealing the origin of postsclerotherapy hyperpigmentation: identification of melanin and hemosiderin as causative pigments in a histopathological study. Phlebology. 2025. doi: 10.1177/02683555251357095. [Epub ahead of print] [PubMed/Source →]
About the Author

This educational article is written and regularly reviewed by Dr Haroun Gajraj, a GMC‑registered vein specialist who has treated thousands of patients with vein disease and has trained many doctors and nurses in microsclerotherapy, shortwave diathermy and related cosmetic vein procedures.
Dr Gajraj is the founder and board member of the British Association of Sclerotherapists.
You can view his current GMC registration and independent patient reviews on iWantGreatCare for further information about his clinical background. It is designed for healthcare professionals and is based on current clinical guidelines, peer‑reviewed research and day‑to‑day practice experience. The information here is general education only and is not a substitute for individual clinical judgement, local protocols or formal training. Clinicians remain responsible for assessing each patient, obtaining informed consent, explaining risks and alternatives, and working within the scope of their professional registration and regulatory guidance.
Subscribe
For regular updates get my weekly newsletter here
© VeinCare Academy | Dr. Haroun Gajraj | veincare.academy
If you found this article useful, share it with a colleague. Leave a comment below with your experience of combination treatment — the field moves forward when practitioners share what actually works in clinic.
*All references in this blog have been checked against publicly available sources (for example, PubMed and official guideline websites), but this is an educational blog post, not a peer-reviewed journal article. Minor discrepancies in author lists, page numbers or indexing details may remain, and readers should always refer to the original publications and current clinical guidelines before making clinical decisions.